Other Addictions
Counseling
Traditional addiction treatment is based primarily on counseling.
Counselors help individuals identifying behaviors and problems related to their addiction. It can be done on an individual basis, but it's more common to find it in a group setting and can include crisis counseling, weekly or daily counseling, and drop-in counseling supports. They are trained to develop recovery programs that help to reestablish healthy behaviors and provide coping strategies whenever a situation of risk happens. It's very common to see them work also with family members who are affected by the addictions of the individual, or in a community in order to prevent addiction and educate the public. Counselors should be able to recognize how addiction affects the whole person and those around him or her. Counseling is also related to "Intervention"; a process in which the addict's family requests help from a professional in order to get this person into drug treatment. This process begins with one of this professionals' first goals: breaking down denial of the person with the addiction. Denial implies lack of willingness from the patients or fear to confront the true nature of the addiction and to take any action to improve their lives, besides of continuing the destructive behavior.
Once this has been achieved, professional coordinates with the addict's family to support them on getting this family member to alcohol drug rehabilitation immediately, with concern and care for this person. Otherwise, this person will be asked to leave and expect no support of any kind until going into drug rehabilitation or alcoholism treatment. An intervention can also be conducted in the workplace environment with colleagues instead of family.
One approach with limited applicability is the Sober Coach. In this approach, the client is serviced by provider(s) in his or her home and workplace — for any efficacy, around-the-clock — who functions much like a nanny to guide or control the patient's behavior.
Neuropsychology
Cognitive control and stimulus control, which is associated with operant and classical conditioning, represent opposite processes (i.e., internal vs external or environmental, respectively) that compete over the control of an individual's elicited behaviors. Cognitive control, and particularly inhibitory control over behavior, is impaired in both addiction and attention deficit hyperactivity disorder. Stimulus-driven behavioral responses (i.e., stimulus control) that are associated with a particular rewarding stimulus tend to dominate one's behavior in an addiction.
Stimulus control
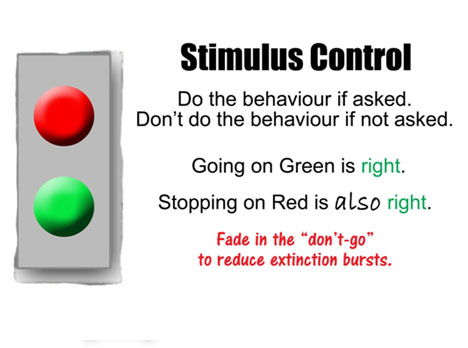
In behavioral psychology, stimulus control is a phenomenon that occurs when an organism behaves in one way in the presence of a given stimulus and another way in its absence. Any stimulus that modifies behavior in this manner is referred to as a discriminative stimulus. Stimulus control of behavior occurs when the performance of a particular behavior is controlled by the presence or absence of a discriminative stimulus. For example, the presence of a stop sign (a discriminative stimulus) at a traffic intersection increases the probability that "braking" behavior will occur.
Some theorists believe that all behavior is under some form of stimulus control. For example, in the analysis of B. F. Skinner, verbal behavior is a complicated assortment of behaviors with a variety of controlling stimuli.
Cognitive control of behavior

Executive functions (collectively referred to as executive function and cognitive control) are a set of cognitive processes that are necessary for the cognitive control of behavior: selecting and successfully monitoring behaviors that facilitate the attainment of chosen goals. Executive functions include basic cognitive processes such as attentional control, cognitive inhibition, inhibitory control, working memory, and cognitive flexibility. Higher order executive functions require the simultaneous use of multiple basic executive functions and include planning and fluid intelligence (i.e., reasoning and problem solving).
Executive functions gradually develop and change across the lifespan of an individual and can be improved at any time over the course of a person's life. Similarly, these cognitive processes can be adversely affected by a variety of events which affect an individual. Both neuropsychological tests (e.g., the Stroop test) and rating scales (e.g., the Behavior Rating Inventory of Executive Function) are used to measure executive functions. They are usually performed as part of a more comprehensive assessment to diagnose neurological and psychiatric disorders.
Cognitive control and stimulus control, which is associated with operant and classical conditioning, represent opposite processes (i.e., internal vs external or environmental, respectively) that compete over the control of an individual's elicited behaviors;4 in particular, inhibitory control is necessary for overriding stimulus-driven behavioral responses (i.e., stimulus control of behavior). The prefrontal cortex is necessary but not solely sufficient for executive functions; for example, the caudate nucleus and subthalamic nucleus also have a role in mediating inhibitory control.
Cognitive control is impaired in addiction, attention deficit hyperactivity disorder, and a number of other central nervous system disorders. Stimulus-driven behavioral responses that are associated with a particular rewarding stimulus tend to dominate one's behavior in an addiction.
Behavioral addiction

The term behavioral addiction correctly refers to a compulsion to engage in a natural reward – which is a behavior that is inherently rewarding (i.e., desirable or appealing) – despite adverse consequences. Preclinical evidence has demonstrated that overexpression of ΔFosB through repetitive and excessive exposure to a natural reward induces the same behavioral effects and neuroplasticity as occurs in a drug addiction.
Reviews of both clinical research in humans and preclinical studies involving ΔFosB have identified compulsive sexual activity – specifically, any form of sexual intercourse – as an addiction (i.e., sexual addiction); moreover, reward cross-sensitization between amphetamine and sexual activity, a property in which exposure to one increases in the desire for both, has been shown to occur preclinically and clinically as a dopamine dysregulation syndrome; ΔFosB expression is required for this cross-sensitization effect, which intensifies with the level of ΔFosB expression.
Reviews of preclinical studies indicate that long-term frequent and excessive consumption of high fat or sugar foods can produce an addiction (food addiction). Gambling is a natural reward which is associated with compulsive behavior and for which clinical diagnostic manuals, namely the DSM-5, have identified diagnostic criteria for an "addiction". There is evidence from functional neuroimaging that gambling activates the reward system and the mesolimbic pathway in particular. Similarly, shopping and playing videogames are associated with compulsive behaviors in humans and have also been shown to activate the mesolimbic pathway and other parts of the reward system. Based upon this evidence, gambling addiction, video game addiction and shopping addiction are classified accordingly.