Other Addictions
Reward sensitization
Neural and behavioral effects of validated ΔFosB transcriptional targets |
|||
Target |
Target |
Neural effects |
Behavioral effects |
c-Fos |
↓ |
Molecular switch enabling the chronic |
– |
dynorphin |
↓ |
• Downregulation of κ-opioid feedback loop |
• Increased drug reward |
NF-κB |
↑ |
• Expansion of NAcc dendritic processes |
• Increased drug reward |
GluR2 |
↑ |
• Decreased sensitivity to glutamate |
• Increased drug reward |
Cdk5 |
↑ |
• GluR1 synaptic protein phosphorylation |
Decreased drug reward |
Reward sensitization is a process that causes an increase in the amount of reward (specifically, incentive salience) that is assigned by the brain to a rewarding stimulus (e.g., a drug). In simple terms, when reward sensitization to a specific stimulus (e.g., a drug) occurs, an individual's "wanting" or desire for the stimulus itself and its associated cues increases. Reward sensitization normally occurs following chronically high levels of exposure to the stimulus. ΔFosB (DeltaFosB) expression in D1-type medium spiny neurons in the nucleus accumbens has been shown to directly and positively regulate reward sensitization involving drugs and natural rewards.
"Cue-induced wanting" or "cue-triggered wanting", a form of craving that occurs in addiction, is responsible for the majority of compulsive behavior that addicts exhibit. These cues create overwhelming short-term urges to engage an addictive stimulus by acting as conditioned reinforcers for the addictive stimulus (a primary reinforcer) that are assigned pathologically high levels of incentive salience ("want").
Research on the interaction between natural and drug rewards suggests that dopaminergic psychostimulants (e.g., amphetamine) and sexual behavior act on similar biomolecular mechanisms to induce ΔFosB in the nucleus accumbens and possess a bidirectional reward cross-sensitization effect that is mediated through ΔFosB.
In contrast to ΔFosB's reward-sensitizing effect, CREB transcriptional activity decreases user's sensitivity to the rewarding effects of the substance. CREB transcription in the nucleus accumbens is implicated in psychological dependence and symptoms involving a lack of pleasure or motivation during drug withdrawal.
The set of proteins known as "regulators of G protein signaling" (RGS), particularly RGS4 and RGS9-2, have been implicated in modulating some forms of opioid sensitization, including reward sensitization.
Diagnosis
The 5th ion of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) uses the term "Substance Use Disorder" to refer to a spectrum of use-related conditions. The DSM-5 eliminates the terms "abuse" and "dependence" from diagnostic categories, instead using the specifiers of "mild", "moderate" and "severe" to indicate the extent of disordered use. Specifiers are determined by the number of diagnostic criteria present in a given case. The manual has never actually used the term "addiction" clinically. Currently, only drug addictions and gambling addiction are listed in the DSM-5. Past ions have used physical dependence and the associated withdrawal syndrome to identify an addictive state. Physical dependence occurs when the body has adjusted by incorporating the substance into its "normal" functioning – i.e., attains homeostasis – and therefore physical withdrawal symptoms occur upon cessation of use. Tolerance is the process by which the body continually adapts to the substance and requires increasingly larger amounts to achieve the original effects. Withdrawal refers to physical and psychological symptoms experienced when reducing or discontinuing a substance that the body has become dependent on. Symptoms of withdrawal generally include but are not limited to anxiety, irritability, intense cravings for the substance, nausea, hallucinations, headaches, cold sweats, and tremors.
Medical researchers who actively study addiction have criticized the DSM classification of addiction for being flawed and involving arbitrary diagnostic criteria.74Writing in 2013, the director of the United States National Institute of Mental Health discussed the invalidity of the DSM-5's classification of mental disorders:
The strength of each of the ions of DSM has been "reliability" – each ion has ensured that clinicians use the same terms in the same ways. The weakness is its lack of validity. Unlike our definitions of ischemic heart disease, lymphoma, or AIDS, the DSM diagnoses are based on a consensus about clusters of clinical symptoms, not any objective laboratory measure. In the rest of medicine, this would be equivalent to creating diagnostic systems based on the nature of chest pain or the quality of fever.
Most recently, though, the NIH acknowledged advances in identifying biomarkers, noting they outperform traditional phenomenological categories in identifying types of psychosis. As a diagnostic biomarker, ΔFosB expression could be used to diagnose an addiction in humans, but this would require a brain biopsy and therefore isn't used in clinical practice.
Treatment

According to a review, "in order to be effective, all pharmacological or biologically based treatments for addiction need to be integrated into other established forms of addiction rehabilitation, such as cognitive behavioral therapy, individual and group psychotherapy, behavior-modification strategies, twelve-step programs, and residential treatment facilities."
Behavioral therapy

A meta-analytic review on the efficacy of various behavioral therapies for treating drug and behavioral addictions found that cognitive behavioral therapy (e.g., relapse prevention and contingency management), motivational interviewing, and a community reinforcement approach were effective interventions with moderate effect sizes. Preclinical research using a rodent model of cue exposure therapy (CET) show that this type of treatment is more effective in adults compared to adolescents, however that adolescent outcomes can be improved by acute treatment at the time of (CET) with a dopamine 2 receptor agonist.
Clinical and preclinical evidence indicate that consistent aerobic exercise, especially endurance exercise (e.g., marathon running), actually prevents the development of certain drug addictions and is an effective adjunct treatment for drug addiction, and for psychostimulant addiction in particular. Consistent aerobic exercise magnitude-dependently (i.e., by duration and intensity) reduces drug addiction risk, which appears to occur through the reversal of drug induced addiction-related neuroplasticity. One review noted that exercise may prevent the development of drug addiction by altering ΔFosB or c-Fosimmunoreactivity in the striatum or other parts of the reward system. Aerobic exercise decreases drug self-administration, reduces the likelihood of relapse, and induces opposite effects on striatal dopamine receptor D2 (DRD2) signaling (increased DRD2 density) to those induced by addictions to several drug classes (decreased DRD2 density). Consequently, consistent aerobic exercise may lead to better treatment outcomes when used as an adjunct treatment for drug addiction.
Alcohol addiction

Alcohol, like opioids, can induce a severe state of physical dependence and produce withdrawal symptoms such as delirium tremens. Because of this, treatment for alcohol addiction usually involves a combined approach dealing with dependence and addiction simultaneously.
Pharmacological treatments for alcohol addiction include drugs like naltrexone (opioid antagonist), disulfiram, acamprosate, and topiramate. Rather than substituting for alcohol, these drugs are intended to affect the desire to drink, either by directly reducing cravings as with acamprosate and topiramate, or by producing unpleasant effects when alcohol is consumed, as with disulfiram. These drugs can be effective if treatment is maintained, but compliance can be an issue as alcoholic patients often forget to take their medication, or discontinue use because of excessive side effects. According to a Cochrane Collaboration review, the opioid antagonist naltrexone has short-term efficacy treating alcoholism, but evidence of longer term efficacy is lacking.
Behavioral addictions

Behavioral addiction is a treatable condition. Treatment options include psychotherapy and psychopharmacotherapy (i.e., medications) or a combination of both. Cognitive behavioral therapy (CBT) is the most common form of psychotherapy used in treating behavioral addictions; it focuses on identifying patterns that trigger compulsive behavior and making lifestyle changes to promote healthier behaviors. Currently, there are no medications approved for treatment of behavioral addictions in general, but some medications used for treatment of drug addiction may also be beneficial with specific behavioral addictions.
Cannabinoid addiction
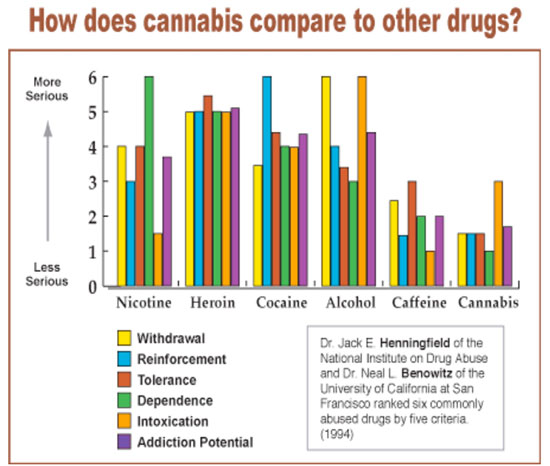
As of 2010, there are no effective pharmacological interventions for cannabinoid addiction. A 2013 review on cannabinoid addiction noted that the development of CB1 receptor agonists that have reduced interaction with β-arrestin 2 signaling might be therapeutically useful.
Nicotine addiction

Another area in which drug treatment has been widely used is in the treatment of nicotine addiction, which usually involves the use of nicotine replacement therapy, nicotinic receptor antagonists, or nicotinic receptor partial agonists. Examples of drugs that act on nicotinic receptors and have been used for treating nicotine addiction include antagonists like bupropion and the partial agonist varenicline.
Opioid addiction
Opioids cause physical dependence, and treatment typically addresses both dependence and addiction.
Physical dependence is treated using replacement drugs such as suboxone or subutex (both containing the active ingredients buprenorphine) and methadone. Although these drugs perpetuate physical dependence, the goal of opiate maintenance is to provide a measure of control over both pain and cravings. Use of replacement drugs increases the patient's ability to function normally and eliminates the negative consequences of obtaining controlled substances illicitly. Once a prescribed dosage is stabilized, treatment enters maintenance or tapering phases. In the United States, opiate replacement therapy is tightly regulated in methadone clinics and under the DATA 2000 legislation. In some countries, other opioid derivatives such as levomethadyl acetate, dihydrocodeine, dihydroetorphine and even heroin are used as substitute drugs for illegal street opiates, with different prescriptions being given depending on the needs of the individual patient. Baclofen has led to successful reductions of cravings for stimulants, alcohol, and opioids, and also alleviates alcohol withdrawal syndrome. Many patients have stated they "became indifferent to alcohol" or "indifferent to cocaine" overnight after starting baclofen therapy.
Psychostimulant addiction
As of May 2014, there is no effective pharmacotherapy for any form of psychostimulant addiction. Reviews from 2015 and 2016 indicated that TAAR1-selective agonists have significant therapeutic potential as a treatment for psychostimulant addictions; however, as of February 2016, the only compounds which are known to function as TAAR1-selective agonists are experimental drugs.
Research
Research indicates that vaccines which utilize anti-drug monoclonal antibodies can mitigate drug-induced positive reinforcement by preventing the drug from moving across the blood–brain barrier; however, current vaccine-based therapies are only effective in a relatively small subset of individuals. As of November 2015, vaccine-based therapies are being tested in human clinical trials as a treatment for addiction and preventative measure against drug overdoses involving nicotine, cocaine, and methamphetamine.
Since addiction involves abnormalities
in glutamate and GABAergic neurotransmission, receptors associated with these neurotransmitters (e.g., AMPA receptors, NMDA receptors, and GABAB receptors) are potential therapeutic targets for addictions. N-acetylcysteine, which affects metabotropic glutamate receptors and NMDA receptors, has shown some benefit in preclinical and clinical studies involving addictions to cocaine, heroin, and cannabinoids. It may also be useful as an adjunct therapy for addictions to amphetamine-type stimulants, but more clinical research is required.
Current medical reviews of research involving lab animals have identified a drug class – class I histone deacetylase inhibitors – that indirectly inhibits the function and further increases in the expression of accumbal ΔFosB by inducing G9a expression in the nucleus accumbens after prolonged use. These reviews and subsequent preliminary evidence which used oral administration or intraperitoneal administration of the sodium salt of butyric acid or other class I HDAC inhibitors for an extended period indicate that these drugs have efficacy in reducing addictive behavior in lab animalsnote 7 that have developed addictions to ethanol, psychostimulants (i.e., amphetamine and cocaine), nicotine, and opiates; however, as of August 2015 no clinical trials involving human addicts and any HDAC class I inhibitors have been conducted to test for treatment efficacy in humans or identify an optimal dosing regimen.